
Welcome to the
Malaysian Family Physician, a peer-reviewed open-access journal of family practice
and primary care research.
CASE REPORT
A CHILD WITH EPISTAXIS, REDUCED HEARING AND CERVICAL LYMPHADENOPATHY: A RARE CASE OF NASOPHARYNGEAL CARCINOMA IN A CHILD
S Muhammad Izani1, M Irfan2, Y Suhaimi1
1Department of Otorhinolaryngology - Head & Neck Surgery, Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia. (Muhammad Izani Shiyuti, Suhaimi Yusof)
2Department of Otorhinolaryngology - Head & Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia. (Irfan Mohamad)
Address for correspondence: Dr Irfan Mohamad, Department of Otorhinolaryngology - Head & Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia, 16150 Kota Bharu, Kelantan. Tel: 09-7676 420, Fax: 06-7676 424, Email: irfan@kb.usm.my
ABSTRACT
Although nasopharyngeal carcinoma (NPC) is common in this part of the world, the incidence among children is still very low worldwide. The diagnosis is sometimes delayed because of the late reporting of the symptom by the patient or parents, or difficulty in reaching the final diagnosis due to its hidden anatomical location. The challenges include the difficult endoscopy in children, inability to differentiate an adenoid from the tumour on radiograph and often the inconclusive fine needle aspiration findings. If the tumour mass at Fossa of Rosenmuller can be clearly appreciated and biopsied with undoubtedly proven histology of NPC, the diagnosis can be straight forward and treatment can be commenced as early as possible. We report a 10-year-old child presented with bilateral neck cervical lymphadenopathy and epistaxis with fine needle aspiration cytology (FNAC) of the neck mass reported as lymphoma. Further work-up confirmed he was suffering from NPC.
Keywords: Nasopharyngeal carcinoma, children, differential diagnosis, management.
Muhammad Izani S, Irfan M, Suhaimi Y. A child with epistaxis, reduced hearing and cervical lymphadenopathy: a rare case of nasopharyngeal carcinoma in a child. Malaysian Family Physician. 2011;6(2&3):82-84
INTRODUCTION
Nasopharyngeal carcinoma (NPC) is one of the commonest tumours in head and neck region. However, the incidence in children is very small. In United States, the annual incidence is 1-2 per million under the age of 30.1 The disease is more common among Asian population.2 Among different ethnic group, Chinese possess the highest risk including Malaysia.3 Similar ethnic risk also applied to adult NPC. The following case illustrates a rare case of NPC diagnosed in a 10-year-old boy.
CASE SUMMARY
MAA, a 10-year-old Malay boy, was referred from district hospital to Ear, Nose and Throat (ENT) Clinic with the problem of painless bilateral neck swelling of two months duration. It was progressively increasing in size. He also had history of epistaxis from both nostrils. There was history of reduced hearing on right side for one month without any other ear complaint. The left ear was normal. There was no history of chronic cough, fever or other constitutional symptoms. There was no family history of malignancy. Physical examination revealed bilateral neck masses located at the level II on both sides (Figure 1). It measured 4 cm x 3 cm on right, and 3 cm x 3 cm on left side. Nasoendoscopy showed fungating mass at the nasopharyngeal region which encroached onto nasal septum and posterior part of inferior turbinate. Otoscopy examination showed bilateral intact tympanic membrane with evidence of fluid inside the middle ear. Tuning fork test and pure tone audiometry revealed bilateral conductive hearing loss.
The patient was initially referred from a district hospital with differential diagnoses of tuberculous lymphadenitis, lymphoma, metastatic carcinoma and juvenile nasoangiofibroma. Full blood picture was obtained and it was normal. Mantoux test was negative. Fine needle aspiration cytology (FNAC) of left neck lymph node showed features of lymphoma. He then was referred to our clinic for further assessment.
Computed tomography (CT) scan of neck showed large aggressive soft tissue mass in the nasopharynx with infiltration of prevertebral muscles as well erosion of pterygoid muscles with extension into right pterygopalatine fossa, ethmoid and sphenoid sinuses (Figure 2). There were multiple enlarged lymph nodes on both sides of upper neck. Chest radiograph was clear and ultrasound abdomen was normal.
Examination under anaesthesia was done and the findings revealed fungating, non-vascular mass occupying 90% of nasopharyngeal region (Figure 3). Biopsy of nasopharyngeal mass was taken and sent for histopathological examination (HPE).
HPE result of the nasopharyngeal mass confirmed features of non-keratinizing carcinoma, undifferentiated type (WHO Type III). He was referred to Oncology & Radiotherapy Unit for further chemoradiation treatment. He was coping well with the treatment and did not show any symptom and sign of recurrence.

Figure 1: Bilateral level II cervical lymphadenopathy
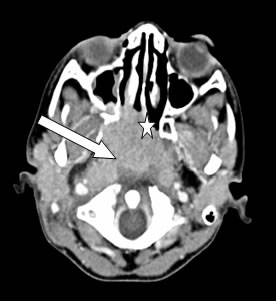
Figure 2: Axial CT scan showed mass at nasopharyngeal region (arrow) with local infiltration to the right posterior inferior turbinate and nasal septum (star)
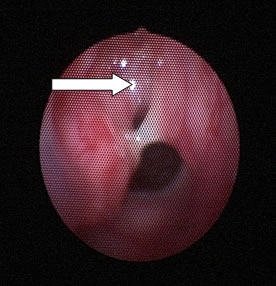
Figure 3: Endoscopic view of nasopharynx from right nostril. Note the nasopharyngeal mass (arrow) which is extended to the posterior end the posterior end of inferior turbinate (8 o’clock position) and the nasal septum (at 3 o’clock position)
DISCUSSION
NPC is a rare disease in children. The common early presenting symptom includes otitis media with effusion (OME).4 In our case, the presenting symptom is bilateral neck swelling which can be due to many causes. For doctors who do not have facilities to examine the intranasal cavity, very often the diagnosis is delayed. More commonly, it is clinically misdiagnosed as lymphoma or tuberculosis.
Epistaxis is known to be the presentation of any neoplasm in the nasal cavity. However, it is not uncommon to have children or teenage with epistaxis without any intranasal pathology. When epistaxis is occurring with the presence of cervical lymphadenopathy, metastatic disease from the primary nasal cavity must be excluded in the early course of management. Cervical lymphadenopathy constituted majority of the presenting symptom of NPC.2
Performing an endoscopy in children with suspected intranasal pathology also impose extra challenges. Besides making the child to stay still for the endoscope to be performed has its own difficulty, the presence of mass in the nasopharynx can be easily mistaken as adenoid, which is a normal structure to be found in children. The enlarged adenoids, which also can be visualized through lateral skull radiograph, can also be the cause of OME and conductive hearing loss (CHL). Both OME and CHL are the known presenting symptoms of NPC. With the presence of cervical lymphadenopathy, the adenoid should be excluded as in this case. The lesion must be biopsied for the confirmation of the disease.
Histologically, NPC can be graded into three types based on World Health Organization (WHO) classification; (Type I) Squamous cell carcinoma (keratinizing) which can be further classified into well, moderately and poorly differentiated; (Type II) non-keratinizing carcinoma; and (Type III) undifferentiated carcinoma.5 In our patient, the histological type is WHO-Type III, which is consistent with world wide report that children are more prone to Type II and III tumour.6
Besides the stage of the disease at the commencement of the therapy, the survival rates for young patients are generally better than in adults.7 The histological Type III which are more common in children possess a higher degree of radiosensitivity and local radiocurability, in addition to their tolerability to radiation better than adults.8
REFERENCES
- Jenkin RD, Anderson JR, Jereb B, et al. Nasopharyngeal carcinoma - a retrospective review of patients less than thirty years of age: a report of Children’s Cancer Study Group. Cancer. 1981;47(2): 360-6. [PubMed]
- Pua KC, Khoo AS, Yap YY, et al. Nasopharyngeal Carcinoma Database. Med J Malaysia. 2008;63(Suppl C):59-62. [PubMed]
- Yadav M, Tan MK, Singh P, et al. Nasopharyngeal carcinoma in Malaysians under the age of 20 years. Clin Oncol. 1984;10(4):353-61. [PubMed]
- Noorizan Y, Chew YK, Khir A, et al. Nasopharyngeal carcinoma: recognizing it early in children with otitis media with effusion. Med J Malaysia. 2008;63(3):261-2. [PubMed]
- Simons MJ, Shanmugaratnam K. The biology of nasopharyngeal carcinoma. A series of workshops on the biology of Human Cancer Report no. 16. Union Internationale Contre Cancer Technical Report Series; 1982. vol 71 p. 3-9.
- Mertens R, Granzen B, Lassay L, et al. Nasopharyngeal carcinoma in childhood and adolescence: concept and preliminary results of the cooperative GPOH study NPC-91. Gesellschaft für Pädiatrische Onkologie und Hämatologie. Cancer. 1997;80(5):951-9. [PubMed]
- Papavasiliou C, Pavlatou M, Pappas J. Nasopharyngeal cancer in patients under the age of thirty years. Cancer. 1977;40(5):2312-6. [PubMed]
- Ong YK, Tan HK. Nasopharyngeal carcinoma in children. Int J Pediatr Otorhinolaryngol. 2000;55(2):149-54. [PubMed]